When Work and Life Cross Paths: Putting Your Best Foot Forward (In Design)
Written By: Kristin Benokraitis, Director of Quality and Operations at Gilero
For the past 12 years I have worked in the medical device industry where I have developed new and exciting products which help to improve patient care, and in many cases, save lives. It’s the kind of thing that makes you want to get up and go to work each day. Over the years I have had friends and family members being treated with medical devices that I have personally worked on, such as a drug-eluting stents. The story I’m about to share is a simple example of how critical human-centric design is, especially as the healthcare environment continues to shift to homecare solutions. It’s also a story about how sometimes a small change in design can make a huge difference in a user’s experience.
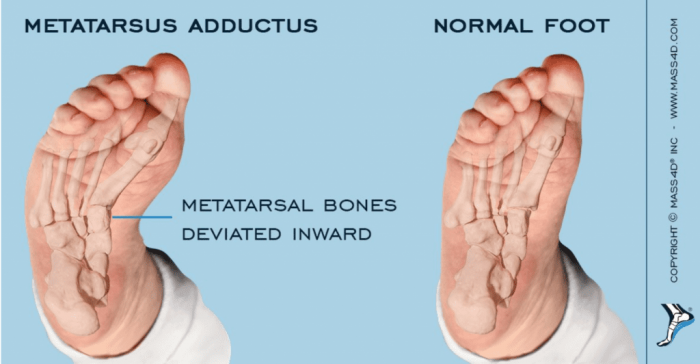
In May 2018, I gave birth to a healthy baby boy. At his one month appointment with our pediatrician, his feet appeared to be curved more than normal and recommended meeting with a local orthopedist for further evaluation. The orthopedist determined he had a medical condition called metatarsus adductus, or a fancy way of saying his feet were curved inward based on a measurement from his inner foot to his second toe. Metatarsus adductus occurs in approximately 1 to 2 per 1,000 births and the cause is unknown. If left untreated, there is an increased risk for developmental hip dysplasia. Initial treatment at his young age involved plaster and fiberglass casts for three weeks. The casts were meant to hold our son’s feet in a specific position, with the hope that they would remain straight due to bone/muscle memory.
The casts were then taken off with a Stryker rotating saw each week to allow for foot measurements and a clean application of a new cast. Although there was some improvement after the casts, further treatment was required: orthotic shoes. The orthotic shoes required an orthopedic technician to set the position of the shoes with an allen wrench. These shoes had to be worn for 23 hours each day – even while he was sleeping.
Lesson #1: Product users are going to screw-up
If feet are pointed inward, like is the case with metatarsus adductus, then it makes sense that the orthotic shoes have to position the foot outward. At some point early on, we (or a family member or daycare worker) inadvertently switched which shoe went on which foot. The mistake continued for 3 months. Imagine the horror being told that, for the past 3 months, you (as parents) were not treating the condition, but possibly making things worse. Let’s pause and think about this for a minute. If you have ever accidentally put the wrong shoe on the wrong foot, not only would it feel weird, but it would immediately look wrong too. Over years of wearing shoes, you become accustomed to seeing the toes of shoes to look a certain way when they are on your feet. Imagine if one day, you had to re-train your brain to ignore the sense of “something doesn’t look right” and start wearing your shoes on the wrong feet all of the time. It is not only outside of normal practice and use cases, but it is the complete opposite.
In this case, the orthotic shoe designer expected the user to adjust their normal behavior to use the product properly. The shoes were not designed to be intuitive for end users (parents), nor was there any indication for which shoe was for the left or right foot. In reviewing the included Instructions For Use (which were later found in the shoe box without our knowing), we noticed that the instructions provided by the American distributor didn’t match up directly with the instructions provided by the Italian manufacturer. The instructions from the manufacturer were translated from Italian to English, leading to further confusion on how to properly put on and use the orthotic shoes.

During development, a utilizing a risk analysis tool such as a Use FMEA (failure mode and effects analysis) could have identified my failure mode – “parents put shoes on wrong feet”. But as engineers, we often put aside what we may think are the most obvious mistakes that a user may use. Because if you give a medical device to an engineer – of course they are going to hold it, open it and use it the right way. Whereas, if you give the same device to Aunt Betty, she immediately flips it upside and tries to use it with the cap still on. It reminds me of the time I was standing in line at a CVS picking up a prescription. An older gentleman in front of me was sharing a story – unprompted – about a time that his wife was giving him an injection in his behind and the needle “just disappeared.” They were so concerned that the needle was left in his body that they called 911. It turns out, they were using a passive needle safety device, where the needle does in fact disappear out of view, but doesn’t end up inside the patient’s body. Now, to the average nurse or doctor, this is common knowledge. To your grandma or grandpa who are using this type of device for the first time, it could mean they think a needle is stuck where the sun don’t shine.
Lesson #2: A change in use case can cause a device to go from treating to hurting the patient

Back to orthotic shoes! Back to putting them on the wrong feet for 3 months! Between the next appointment, our son started crawling. Crawling was fun until he realized it was even more fun to try and stand up. We quickly realized that his shoes were starting to hinder his ability to learn how to stand up. Imagine trying to walk for the first time, but with ice skates. The nice part about the orthotic shoes is an exterior hinge point which allows doctors quick and easy access to adjust the position or angle of the shoe. When our son was non-mobile, this was not a big deal. But as soon as he was able to stand up, the plastic component which housed the hinge feature created an uneven surface on the bottom of the shoe. In fact, it was a significant enough difference that it caused our son to stand mostly on his tippy toes instead of flat footed. Not only that, we feared that it might be slowing his ability to start walking. We didn’t want the shoes, which were intended to treat one medical condition, to be the cause of a different medical condition.
So it’s now over six months after our first orthopedic appointment and we were curious about other orthotic options, given his new stage in mobility. The doctor said that there was a flat shoe version called reverse lace-up shoes; however, they were for infants that were at least 1 ½ years old. So too bad, we were stuck with the shoes we had. The good news was now that the shoes were on the right feet, they appeared to be helping his condition. Our son’s feet measured within “normal” criteria, but to make sure they didn’t revert back, the doctor ordered another 3 months with the orthotic shoes. Sidebar – the reason it was so important to address the condition at his young age with the casts and shoes was because the alternative treatment, if required in the future, would be surgery.
Lesson #3: Small design changes can make a big difference

At this point, my brain was itching to solve the problem. It wasn’t a massive or challenging problem to solve. Rather, it was relatively straight forward. I took measurements of the shoe and talked with our design engineers (Ted Mosler and Darrin Swanson) to think up a solution. Initial brain storming, 3D CAD modeling and a round of prototyping led to “Gen 1” of the shoe covers. The 3D printed shoe cover was attached to the shoe itself, and then a silicone sheet with sticky backing was stuck to the bottom of the shoe cover to offer some traction. The design allowed for future access to the hinge area, which offering a flat surface for our son to stand on.
Lesson #4: The first solution isn’t always the best solution. Test and iterate!

We learned pretty quickly after watching our son in his new “shoes” that there was room for improvement. Isn’t that what the design process is all about? A 3D CAD model might look great on your computer screen, but until you put it in the user’s hands (or feet in this case), opportunities for improvement may not be obvious. In our case the tabs intended to align the shoe cover broke off within hours, and the silicone sheet intended to provide a grippy surface was too “sticky” when in contact with the floor and peeled off. The other interesting observation was our son was compensating for the unevenness of the orthotic shoe while in the standing position. In other words, he had spent enough time standing up on “ice skates” that he trained his body to compensate for it. So when we gave him a flat surface to stand on, it required him to readjust his standing position all over again.
We then took our observations from the Gen 1 prototypes (even after just a single day’s use) to update the design to the Gen 2 model. Design revisions included modifying the geometry and changing the prototyping material. Our lab has the ability to 3D print both rigid and elastomeric materials. To give the shoe cover more of a “sneaker sole” feel, we decided to make the Gen 2 prototypes out of the softer material, which eliminated the need for the silicone sheet.
A few weeks later, we showed the orthopedist and a few residents the Gen 2 prototypes. Not only did they think they were awesome, they wanted to know how we made them. We will continue to use the prototypes until he no longer has to wear his orthotic shoes, and this story will be documented in his baby book and shared over the dinner table for future laughs.
Lesson #5 (Bonus): They don’t make a baby wipe that can clean baby poop off of plaster casts
Just when you think changing a diaper is difficult enough, the world throws a new challenge at you. Try changing a diaper on an infant who has two legs in casts up to the hip area. We learned the hard way that trying to clean a plaster cast doesn’t work. Maybe we will tackle this product next!
Ready to turn your idea for a medical or drug delivery device into a reality?
Talk with an expert today.